ANTERIOR CRUCIATE LIGAMENT (ACL) RUPTURE
Anterior Cruciate Ligament Injuries are
relatively common in dogs. This article
will discuss what the problem is and how we fix it.
THE KNEE JOINT IS A VERY COMPLEX STRUCTURE
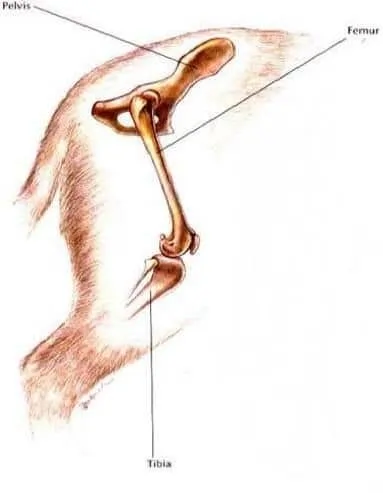
In dogs, this joint is sometimes called the stifle. The end of the thigh bone, or femur, rests precariously on the top of the tibia, or lower leg bone. The ends of each bone are covered with a thin layer of cartilage called articular cartilage. There is a cartilage pad called the meniscus in between to cushion the bone ends. The whole thing is held together by ligaments.
OF PARTICULAR INTEREST IS THE CRANIAL CRUCIATE LIGAMENT.
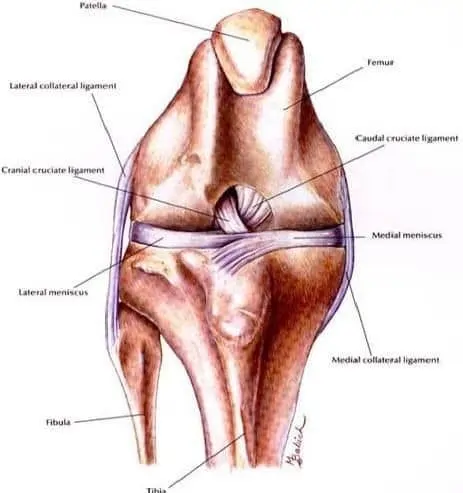
There are two cruciate ligaments. They are named “cruciate” because they cross each other. They are located inside the joint in between the femur and the tibia, and together they keep the femur sitting squarely on top of the tibia. One of the cruciate ligaments is located more to the front, and is called the anterior cruciate ligament. It is an annoying bit of anatomical tradition allows this ligament to be called either the cranial or the anterior cruciate ligament. In veterinary medicine, it is generally called the anterior cruciate ligament and is often abbreviated ACL. Its partner is the caudal cruciate ligament.
WHAT HAPPENS WHEN ONE OF THE CRUCIATE LIGAMENTS BREAKS?

THERE ARE TWO REASONS THE ACL CAN BREAK
The first resson is for a healthy ACL to be severely traumatized. The trauma can be a mis-step, a fall, a twist, or a sudden wrench. This would be a the kind of injury that happens to football players. We see this type of acute injury most commonly in young, athletic dogs, and it typically happens while they are exercising.
The other way an ACL can fail is by slow degeneration. In some middle-aged, somewhat overweight, less active dogs, the ACL will begin to degenerate slowly over years. Eventually the ACL fails entirely, and failure may occur during something as non-stressful as a walk around the block or getting up. Often, these knees will have developed advanced arthritis before the ACL ever fails. These dogs often rupture the ACL in the other leg within a few years as well. In my practice, the slow, degenerative ACL injuries outnumber the acute traumatic ACL injuries.
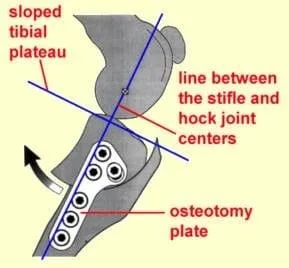
KNEE CONFORMATION PLAYS A MAJOR ROLE
It is thought that poor knee conformation is the root cause of most ACL ruptures, especially of the slow degenerative 
THIS FORMS THE BASIS FOR ONE METHOD OF ACL RUPTURE TREATMENT.
The surgeons who pioneered this technique, in a highly controversial move, actually patented the procedure, and then made a fortune selling equipment and running training schools. Although the patent has now expired, because of the technical nature of the procedure and the expensive instrumentation required, it still is mainly done by Board Certified specialist surgeons. It has the advantage of a fairly rapid recovery and in general good results, especially in larger or more active patients, but has the disadvantage of being more costly to perform. Most referral surgeons charge somewhere in the neighborhood of $2,000 to $3,000 to perform a TPLO.
ARTIFICIAL LIGAMENT IMPLANTATION: THE TIGHTROPE TECHNIQUE

AN IMPORTANT PART OF EITHER SURGERY IS THE EXAMINATION OF THE MENISCUS
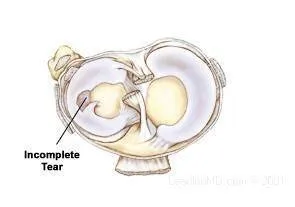
The operated area heals by forming fibrocartilage, which is a version of scar tissue. It is not as good as the original meniscus, but it is better than leaving the torn
meniscus. It takes some time for this healing to happen, so that joints with a torn medial menuscus heal slower, and the final result is not as good as in joints without a torn
meniscus.
SO WHICH TECHNIQUE IS BETTER?
When the TPLO was first introduced, it was claimed that the TPLO technique was better in all situations. However, as our experience with other techniques increases, the
research studies are starting to show that TPLO and LI do not differ that much, and patients can having either technique can experience excellent results. The advent of the new
Tightrope technique makes the picture even less clear. Although there are lots of opinions out there, my opinion is that the jury is still out on this one. Both
techniques, the TPLO and theTightrope, can be used on most dogs with excellent results.
However, there are some situations where there is a clear choice. Almost everybody agrees that the TPLO is best for very large dogs (75 pounds and up), and for meduim and large dogs
that are very active. Also, dogs that have an abnormally steep tibial plateau angles do betyter with the TPLO. And almost everyone agrees that the LI technique is best for
small dogs, say 45 pounds and down. The Tightrope technique shows promise in some of the larger dogs as well. I believe the Tightrope is an acceptable alternative
for even large dogs when financial constraints prohibit the TPLO procedure, although the chances of having a less-than-ideal outcome are higher the bigger the dog gets, the more
active he is, or the steeper the tibial plateau angle gets. There are some practitioners who disagree with this opinion.
The real problem is which technique is better for the dogs in the middle, who weight from 45 to 75 pounds. Again, there are lots of opinion out there. My personal opinion is
that TPLO is slightly better than LI for these dogs, and if finances are not an issue I recommend TPLO. The bigger your dog is, the more active he is, or the steeper the
tibial plateau angle, the more strongly I recommend TPLO. However, TPLO can cost twice as much, and I do not feel that it is twice as good for some dogs in this weight range.
I have had excellent success with the Tightrope technique in many dogs this size. With the older LI techniques, the dogs regain good function within two months. With the new
Tightrope technique, many dogs walk out of the clinic the day after surgery with less pain than they walked in. With TPLO, the recovery is quicker than the old LI techniques, but
not always as fast as the Tightrope.
EVERY TECHNIQUE HAS ITS HORROR STORIES
With the TPLO, because the tibia bone is actually sawn in half and plated back together, if something happens to the plate there will be big problems. Things like implant infection, screw failure, or plate failure can lead to limb-threatening complications. You could end up with a bone that can not be re-plated. Because the ACL is never actually replaced, the TPLO has a somewhat higher incidence of meniscus problems post-op.
With the Tightrope, the main complications are implant loosening and implant infection. The Tightrope is more prone to implant infection that the TPLO is. However, the worst thing that can happen with the Tightrope is that if things do not work out well, the implant can be removed and a TPLO can then be performed to improve the situation.
TIGHTROPE POST-OP CARE
Post-op care consists of controlled activity. Knee surgery is all about physical therapy. Many physician surgeons have their knee patients walking the day of surgery, and
so do we. We want our patients to be up and walking, but not putting stress on their new knees. Most dogs will carry the leg for days to a few weeks, gradually starting to
touch the toe down, then gradually bearing more and more weight as the weeks pass. We want early, active movement but no excessive strain. This means that our ACL patients
should be free to walk around the house, but can't run, can't climb or go down flights of stairs, can't jump up and down from furniture, and can't be allowed outside without being on
a leash for the first month. We will allow leash walks the first month as soon as their progress allows. The second month is usually spent gradually increasing their
activity.
THE BOTTOM LINE
While the question of which procedure is best for a given patient is far from clear, there are a few things that we know for sure:
- Dogs with ACL ruptures do much better with surgery than without.
- With either technique, most dogs (90% or better) return to normal function.
- Dogs with acute ACL tears do best, while those dogs with chronic ACL degeneration and tears often have significant arthritis at the time of surgery which never goes away.
- Dogs with abnormally high tibial plateau angles do best with the TPLO
- Big dogs (over 75 pounds), overweight dogs, and very active dogs do best with the TPLO
- The research studies have failed to show any significant differences, on the whole, between techniques.
- Both techniques have complications at about the same rate, but the TPLO complications can be more severe.
- The TPLO costs about twice what the Tightrope costs, more if you include the trip or trips to the referral Surgical Center.